1801006020 - Long case
24 yrs old male came to the medicine OPD with cheif complaint of unstable gait and tremors since 10 days
HISTORY OF PRESENT ILLNESSES
Patient was apparently asymptomatic 12 years ago he started drinking alcohol after his mother passed away in a tragic accident , to alleviate that stress.
He started taking alcohol in the form of ARRACK drinking every alternative day about 1-2 glasses a day
Over the next few months his consumption gradually increased to 3 glasses a day further to 6 glasses a day.This continued upto 5 years after he started drinking .
Around 5 years later he shifted to WHISKY due to ARRACK being banned by the government.He drink around 2 units of whisky daily before going to work and upon returning in the evening he used to feel tired thus used to drink again.
In a few months time his drinking increased upto 12 units a day .
patient also started chewing tobacco since the last 9 years , around 1 packet every 2-3 days
He also complains of sleep disturbances,decreased appetite and sweating if he does not consume alcohol .
Patient has visual hallucinations , pins and needle sensations
His family then enrolled him in a deaddiction programme
no history of any psychiatric conditions .
no history of any head injury .
no history of any loss of consciousness.
no history of any epilepsy.
no fever , vomitings , neck stiffness
DAILY ROUTINE
patient wakes up at 5 in the morning and freshens up and does all his household chores then has a small glass of alcohol following which he goes to work as a an auto driver , he returns home at around 2 to have lunch and takes another 1-2 glasses of alcohol and goes back to work then he comes back home to have dinner at about 9 and sleeps thereafter
patients family members claim that he sneaks out at night to consume more alchol and gets into physical altercation with his family frequently when confronted
PAST HISTORY:
Not a known case of hypertension, diabetes mellitus , epilepsy, asthma ,tb , cad , cvd , thyroid
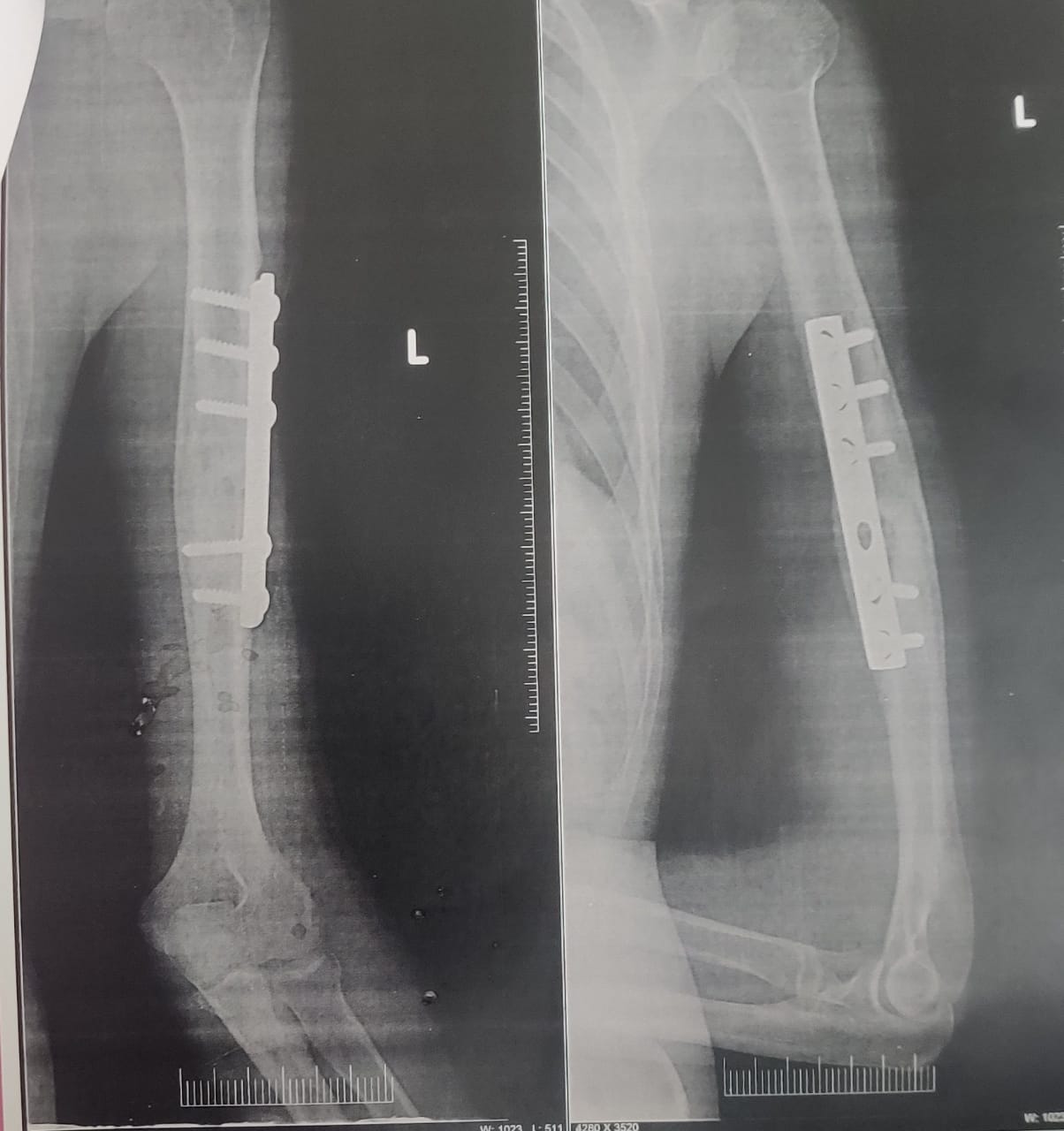
Patient has a history of fracture to the left arm following an accident, it is fixed with a DCP plate .
PERSONAL HISTORY :
Appetite - normal .
Diet - mixed , inadequacy in nutrition.
Sleep - disturbed .
Bowel and bladder movement- regular.
Addictions : alcohol consumption since the age of 11 years .
chewing of gutka since the age of 11 years .
Allergies : No allergies .
GENERAL EXAMINATION:
Patient was examined after taking consent in a well lit room .
Patient is conscious ,coherent , cooperative , oriented time , place and person .
Poorly Built and poorly Nourished .
Temp: Afebrile
BP : 130 / 90 mmHg
PR : 87bpm
RR : 18 cpm
Pallor : absent
Icterus : absent
Cyanosis: absent
Clubbing : absent
Generalized Lymphadenopathy : absent
Bilateral pedal Edema : absent





SYSTEMIC EXAMINATION:
CNS :
Higher mental functions
Conscious , oriented to person , place and time .
Speech : slightly slurred
Memory: intact
Visual hallucinations present
No delusions
No emotional liability
MMSE score - 27/30
CRANIAL NERVE EXAMINATION:
1st : Normal
2nd : visual acuity is normal
3rd,4th,6th : restricted ocular movements .
pupillary reflexes present.
Nystagmus - present .
5th : sensory intact
motor intact
7th : normal
8th : No abnormality noted.
9th,10th : palatal movements present and equal.
11 th : intact
12 th : normal
Motar examination
RT LT
UL LL UL LL
Bulk : Normal Normal Normal Normally
Tone : Normal Normal Normal Normally
Power : 5/5 5/5 5/5 5/5
Reflexes : biceps: present present present
Triceps : present present present
Knee: present present present present
Ankle : present present present present
SENSORY EXAMINATION:
SPINOTHALAMIC SENSATION:
Crude touch : Normal
pain : Normal
temperature : Normal
DORSAL COLUMN SENSATION:
Fine touch : normal
Vibration : normal
Proprioception : normal
Rombergs sign : negative
https://youtube.com/shorts/Y6CGqh_wrII?feature=share
CORTICAL SENSATION:
Two point discrimination : normal
Tactile localisation : normal
CEREBELLAR EXAMINATION:
Slight tremors are present
Truncal ataxia - present
Gait ataxia - present
Nystagmus- present
https://youtu.be/8U4NCKl60-w
Coordination - Finger nose test - slightly altered
Heel knee test - slightly altered
Dysdiadochokinesia - absent
https://youtube.com/shorts/LUSDgPWYsSo?feature=share
GAIT: https://youtube.com/shorts/x0k9rWWj06I?feature=share
wide based gait, swaying to sides ,
Unsteady with a tendency to fall.
unable to perform tandem walking.
SIGNS OF MENINGEAL IRRITATION:
Neck stiffness - absent
Kernigs sign - absent
Brudzinskis sign - absent
CVS :
Apex at normal position
S1 S2 + ,no murmurs
Respiratory system :
chest shape normal
Trachea central
Bilateral air entry Present
Non vesicular breath sounds present
P/A : Soft and Non tender
No organomegaly
Investigations
Hemogram
Hb - 12 gm/dl ( normal =13-17 )
Total count - 10,200 ( normal 4000 - 10000)
Lymphocytes- 18 ( normal 20-40)
Pcv - 37.7 ( normal 40 - 50)
RBC count-3.89 million ( normal 4.5 - 5.5 )
Liver function tests
Total bilirubin- 1.32 mg/dl ( normal 0-1)
Direct bilirubin- 0.34 ( normal 0 - 0.2 )
Alkaline phosphate -185IU/L ( normal 53 - 128 )
Renal function test
Creatinine- 1.4 mg/ dl ( normal 0.9 - 1.3 )
Echo :
Normal size liver with increased ecogenicity and partially distended gallbladder
Chest x ray:


Provisional diagnosis
1. Wernickes encephalopathy ( vit b1 deficiency)
2. Cerebellar degeneration secondary to alcohol consumption
3. Alcohol withdrawal delirium
Treatment
1. Tab lorazepam 2mg
2. Tab benfothiamine 100mg bd
3. Tab baclofen 20mg od
4. Nicotine gums 2 mg
5. Counselling



Comments
Post a Comment